

Can cleaning the air make it harder to breathe?
Can cleaning the air make it harder to breathe?
Well-intentioned policies to fix the ozone layer have been largely successful, but patients with asthma have paid a price.



A win for Earth’s atmosphere
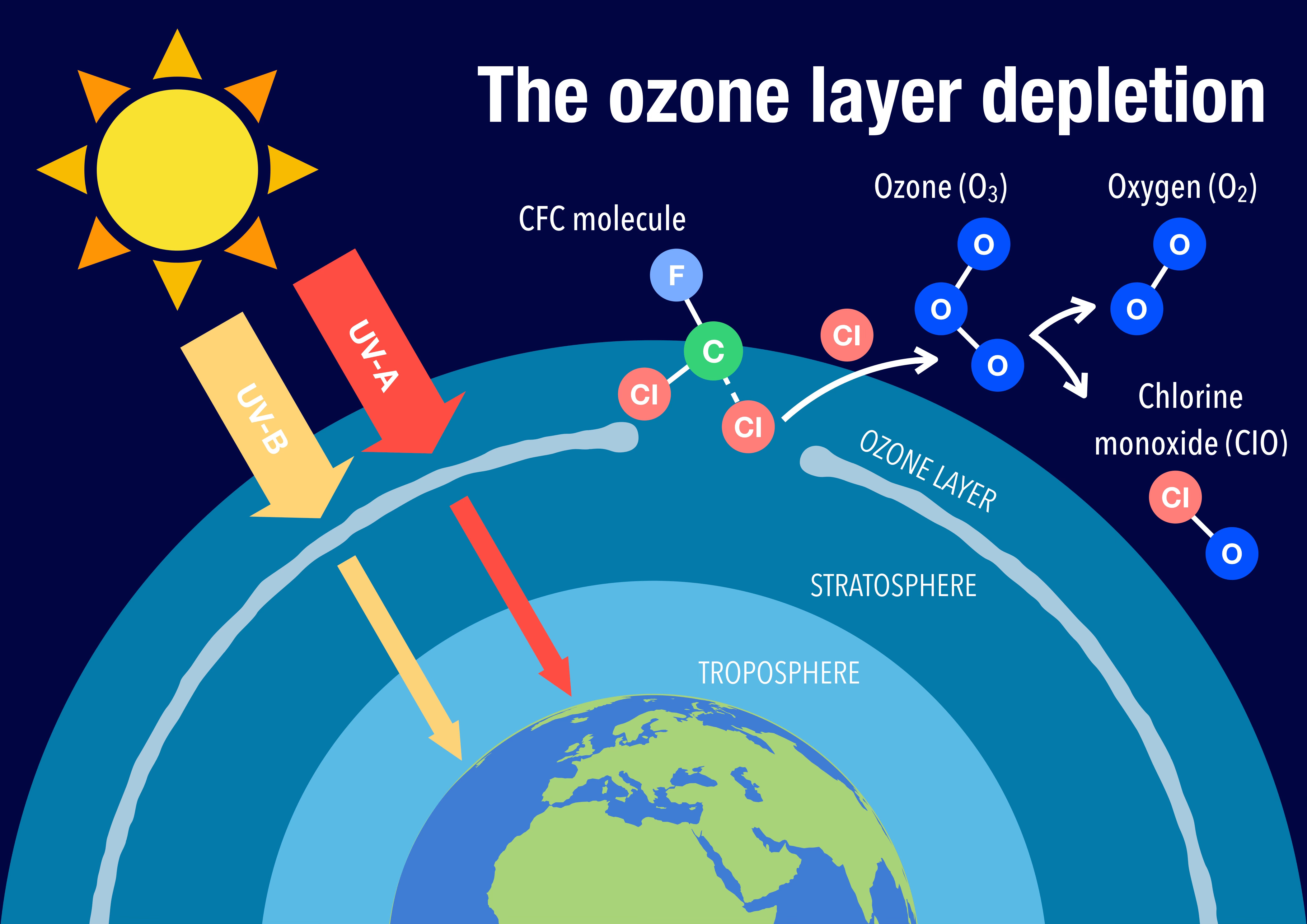
By the 1980s, there was mounting evidence that some chemicals used as refrigerants, solvents, and propellants—such as the ones used in asthma inhalers—were leading to depletion of ozone in the atmosphere. Upon reaching the upper layers of the atmosphere, these “ozone depleting substances” like chlorofluorocarbons (CFCs) catalyzed a chemical reaction that breaks down ozone (O3) into gaseous oxygen (O2).
Ozone plays an important role in blocking harmful ultraviolet (UV) light from entering Earth’s atmosphere; when depleted, more harmful UV reaches the surface, where it can cause health problems like skin cancer and cataracts as well deleterious effects on agriculture and the ecosystem.
In 1987, an international agreement (The Montreal Protocol) was signed to phase out the production of these chemicals to prevent further ozone depletion and allow for levels to rebuild in the atmosphere. CFCs were to be replaced with other substances that would not pose a threat to the ozone layer. The agreement was signed into U.S. law in 1988, upon which President Ronald Reagan said:
“The Montreal Protocol is a model of cooperation. It is a product of the recognition and international consensus that ozone depletion is a global problem, both in terms of its causes and its effects. The protocol is the result of an extraordinary process of scientific study, negotiations among representatives of the business and environmental communities, and international diplomacy. It is a monumental achievement.”
Since then, every member of the United Nations has signed on to the agreement, worldwide production of ozone depleting substances has fallen dramatically, and atmospheric ozone levels are increasing.
The story of the successful international effort to address the ozone layer—a global problem requiring a global solution—has served as an inspiration for other worldwide environmental and climate efforts.
But one group has paid a bigger price, literally, to help the atmosphere: patients with asthma and COPD.
Breathing easier?
Chlorofluorocarbons (CFCs) were one of the most widely used “ozone depleting substances” that were targeted by the Montreal Protocol. While also used as refrigerants (for example, Freon), CFCs were also commonly used as propellants when aerosolizing chemicals, including drugs like albuterol, the active drug in “rescue” inhalers. Aerosolizing the drug into very small particles using a propellant helps the drugs reach deep into the lungs to open up patients’ small airways, making it easier to breathe.

Originally, albuterol inhalers were considered exempt from the ban on CFCs under the Clean Air Act as they were considered medically necessary. But as a new, ozone-safe propellant (hydrofluoroalkane, or HFA) started to be used in inhalers, the FDA ruled that CFC-containing inhalers must be phased out by the end of 2008.
The problem for patients who use inhalers? Before being banned, CFC-propelled inhalers were available as lower-cost, generic drugs. Meanwhile, the new HFA-propelled inhalers were under patent and available only as more expensive, branded drugs. Suddenly, albuterol inhalers became more expensive.
Initial estimates suggested that out-of-pocket costs for albuterol inhalers would increase by about $30 per inhaler. If that was the case, patients might try to conserve their use of albuterol to save money—perhaps at a cost to their health.
What happened?
The HFA-propelled inhalers were indeed more expensive. But a 2016 study by Bapu and several colleagues estimated that the increase in out-of-pocket cost ended up not being as bad as predicted, with the increase being closer to $12 (going from about $13.60 in 2004 to $25.00 in 2009). The analysis also estimated modest reductions in inhaler use with that increase in patient costs: for every $10 increase in out-of-pocket costs, there was about 1 percentage point less inhaler use for adults, and about half a percentage point decrease for children.

Another similar study that focused on children suggested an average monthly increase in cost of about $6 (a figure that is consistent with the other estimate, since patients often don’t use up an entire inhaler in one month). There were no differences in inhaler use among the children despite the price change.
In both of these studies, there was no increase in asthma-related adverse outcomes, like emergency department visits or hospitalizations. So at least when it came to measurable adverse events, it seemed that the hike in albuterol inhaler prices wasn’t stopping patients, on average, from buying it or using it.
What does this mean for the future?
While it’s fortunate that, on average, price increases weren’t that high, inhaler use was barely curbed, and people didn’t seem to be ending up in the hospital with asthma, that doesn’t mean that no patients with asthma suffered as a result of the price increases.
Even the small reductions in albuterol use suggest some patients with symptoms were “toughing it out” and enduring difficulty breathing that they would have treated had it been less expensive to do so. Spending more money on a necessary inhaler means there’s less money for other necessities which could have non-health impacts outside of what these studies could reasonably measure. It’s also hard to know if there are any broader, long term harms of the price increase—the CFC ban presented unique circumstances where patients had to pay more for a decades-old, common, routine medication (the FDA approved the first generic HFA-propelled albuterol in 2020).
We find the inhaler piece of the Montreal Protocol’s story to be fascinating—a prime example of just how far reaching various policy decisions can reach into many aspects of our daily lives. And while this is a fairly unique series of events, we should anticipate and study far reaching consequences, including impacts on health, as we shape environmental policy to manage rising global temperatures.
Ohh, I've but purchased an inhaler since the new type has been available. I only use mine occasionally when I've got a bad cold. So maybe 5 puffs a year, or sometimes I forget where mine is and go a year or two editor it.
But they've been so cheap, I've not had to worry that if I had any issues, I'd just buy a new one.
I'm hoping my two sons won't develop asthma. But yeah, it's an interesting edge case to the ozone story and one I'd not heard about before.