


What makes a doctor a "Likeable Badass"?
In an interview with behavioral scientist Dr. Alison Fragale, we explore ways in which professionals can upend biases that are stacked against them

As a behavioral scientist, University of North Carolina business professor Dr. Alison Fragale has studied power, status, and influence within organizations. It’s no secret that when it comes to power, status, and influence, the deck is stacked against women across a wide variety of organizations and professions, including medicine.

Progress is slow, of course, and waiting for biases to go away simply isn’t an option for those who are currently impacted by them. When she’s not doing research, Fragale works with organizations and the professionals within them, focusing on evidence-based ways to avoid some of the harms brought on by gender-based and other biases. This is why she set out to give women—or really anyone whose talents, expertise, or accomplishments go overlooked and undervalued—a guide to navigating workplace bias in her new book Likeable Badass: How Women Get the Success They Deserve.

When I asked if she’d be up for an interview, I warned her that I was particularly interested in picking her brain about women in medicine. We only scratched the surface of some of the issues women physicians face in the Random Acts of Medicine book (now in paperback!) in the chapter titled “What Makes a Good Doctor?”, so I was excited to get to explore the topic with an expert who could also give some practical advice. Our conversation has been edited for brevity and clarity.
Chris Worsham: At the beginning of Likeable Badass, you quickly acknowledge that when it comes to the role of various biases on status and influence within organizations, the current state of affairs is not great, and it should change. But you go on to say that it’s not going to change as fast as anyone would like, so I’m going to give you the current lay of the land, the science behind it, and some actionable steps you can take to deal with it.
Alison Fragale: Yes, and I think a medical analogy here—although it’s not in the book—is pretty apt. Patients inherit or end up with all kinds of problems that are not their fault and that are difficult to manage. We have people in medicine that say that someday, that problem shouldn’t be a problem—e.g. we should end deaths from cancer or heart disease—and they’re working on solving that. But it doesn’t mean that if you’re the person with cancer or heart disease that you’re just going to throw your hands up in the air and wait for someone else to find a cure.
You’ll say, well, what are the things that are within my control right now to take this thing that I sure as hell don’t deserve and have the best possible outcome I can? That’s how I think about any kind of systemic exclusion or bias and helping someone find what is in their control to be seen the way they deserve to be seen.
CW: That sounds like a pretty good analogy to me. The other thing I discovered as I got into the book—and you make this quite clear—is that a lot of what you talk about is not just applicable to women.
AF: Correct, the science is applicable to everybody. I wrote the book for women because it’s an audience I care about, and if I didn’t write this book, it wasn’t going to get written—and I can write for whoever I want! And I didn’t do this in a devious way, but I just thought wouldn’t it be cool if there were some secrets of the universe and we only told women? Wouldn’t that be awesome?
But no, it’s not just applicable to women. Status is a fundamental human need, something that all human beings care about. In any given situation—regardless of one’s gender, race, sexual identity, any of those characteristics—you go into some rooms and you’ll be the high status person, and you’ll go into the next room and you’ll be the low status person.
As a physician, for example, you could walk into a patient’s room and feel like you’re the high status person in that relationship. But then you go to your conference, and maybe you haven’t been practicing that long, and you’re talking to people who are world renowned people in your field, and you feel like a low status person.
So status is something all human beings contend with, and all the same rules ultimately apply. So no, there is nothing in there that is uniquely women specific that only women have to think about or worry about.
CW: You talk about status, and in the book you delineate the difference between “status” and “power.” What are those differences, broadly speaking?
AF: Status is the extent to which you are respected and highly regarded by other people. Power is the extent to which you control resources that people find valuable. Information is a resource, money is a resource. Car keys for your teenager is a resource. Any time you control a resource that someone else wants, you have power.
Status and power are both sources of influence. Someone will be more likely to be swayed by you and do what you want them to do if they respect your status. But they’ll also do it if you control a resource they value, even if they don’t respect you—like a teenager saying “well I gotta do what mom says, otherwise I don’t get the car.” So they are similar in that regard.
They differ in their consensual nature. Someone’s status is real and can be very far reaching, but status exists only in someone else’s mind. You only get as much status as other people think you should get. It cannot be stolen or taken, only given.
Power is also generally given, but it can also be taken or held by people even if other people don’t necessarily want someone to have it. So the one really important difference between status and power is that everyone gets a say in conferring status to someone, whereas with power, once you have the resources, they may not be able to be take it away from you.
Status has to be continually earned, and I think that’s why it feels amorphous for people and daunting to think about. What I try to do in the book is make it feel more formulaic and less daunting by breaking down the science of how it happens.
CW: What’s a good example of this?
AF: You’re a doctor, right? You’re the only one who can run and interpret a test, the only one who can prescribe medications. You have a lot of resources that patients want. You might also be very respected by your patient. There’s a certain kind of power and status relationship right there.
Where it can start to come apart is when the doctor becomes a patient. When you are a physician treating another physician, they can’t treat themselves but know just enough to be able to put your status into question. They might not honor your usual status because they think “I could be doing this.” You can think of how that situation might be really hard to navigate.
CW: Indeed.
AF: A physician-nurse relationship is another example. The physician is highly dependent on the nurses, so they might have a lot of power over the physician. But then there’s a status differential, since most of the world sees a doctor as a higher status than a nurse. That can put nurses in a situation of being in what we call “low status power holders.” They have a lot of control, but they’re not as highly regarded; this has been a topic of my research. People in these positions do face a lot of incivility—low level mistreatment like having their judgment questioned, cutting them out of information flow, or devaluing their work. And it can even lead to high intensity things like harassment.
And what happens? At least in non-medical contexts, we see very highly qualified people leaving organizations. In fact, senior women leave at higher rates than junior women in organizations, because when you have power and you don’t have status, people mistreat you. And when people mistreat you have options, you’re like “I’m outta here.”
So thinking about honoring people’s status is one of the most controllable, important things we can do to create a workplace that people want to work in. We may be unaware of how our judgments of their power and status are causing us to devalue them, but they are very aware.
CW: You’re reminding me of a study by University of British Columbia economist Heather Sarsons that looked at differences in how male and female surgeons were treated by other doctors who referred their patients to them. In the study, she looked at what happened after a surgeon had a bad outcome—a death following a procedure. If a male surgeon had a bad outcome, it didn’t really change referral rates to that surgeon. But if a female surgeon had a bad outcome, referral rates to her subsequently dropped [see image below].
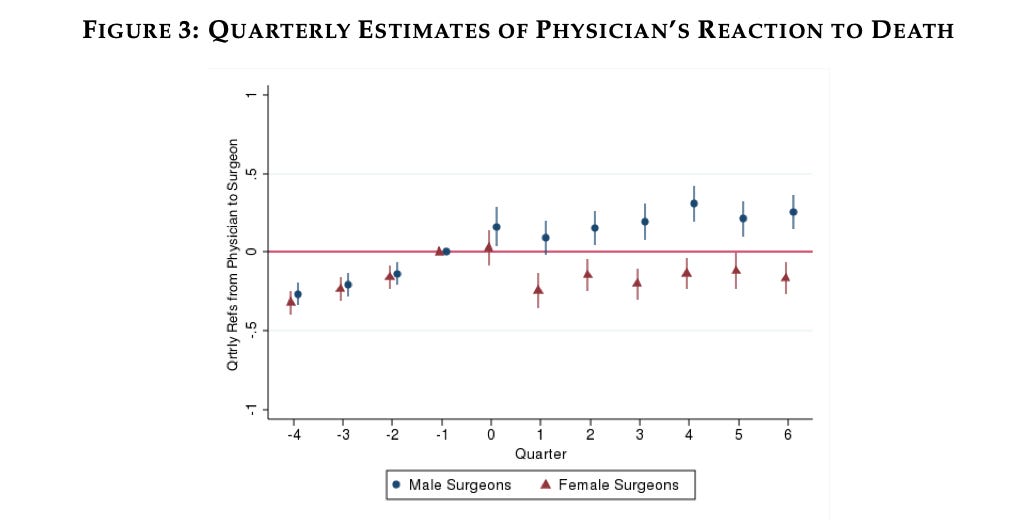
Sarsons’ study suggested that there was an attitude of “it’s not your fault, bad outcomes sometimes happen” with the male surgeons, but for female surgeons the attitude was more likely to be “this is your fault, and I’m not going to send more patients to you.” I imagine this is subconscious in many cases, but is this a difference between “power”—since the male and female surgeons have control over the same resources—and “status,” since male surgeons were afforded the benefit of the doubt while female surgeons weren’t?
AF: That’s right. Because with status comes assumptions of competence and benevolence. So if you have a person that is assumed to be competent and benevolent—let’s say because of their gender—then confirmation bias kicks in. It’s pretty easy to ride that bias. If I think you’re competent, then even competent people can make mistakes, right?
Without status, we tend to assume either competence or benevolence, but not both. Lacking either one is bad when a mistake is made: either you’re not smart enough, or you don’t care enough.
Now, that happens on average, because gender is a status characteristic on average. But if one were look at the distribution of those male surgeons and female surgeons, there will probably be a tail of female surgeons that are getting referred to just as often as the men. So yes, on average the women aren’t getting referred to as often after a complication, but let’s look at the women who that didn’t happen to. I would bet money that the ones who didn’t lose referrals after a complication are seen as highly respected by referring physicians, for some reason or another, because of how they have shown up over the course of their career. So what I would say to any given woman—surgeon or not—is take steps to put yourself in that tail.
Gender is not anyone’s fate. Status is determined by many, many variables, most of which are within our control. My guess is that the surgeons who didn’t lose referrals were good—perhaps in ways that they couldn’t articulate—at navigating their status, such that by the time that bad outcome happened, they were just as respected as the male surgeons and didn’t suffer the same fate as their female colleagues.
CW: That brings us back to this notion of a “likeable badass” as someone who is competent—a badass—and has high status to go along with it. Now, I’m an internist and so I don’t do major procedures, but I do get to suggest to my patients which surgeons they should go to. And I think many of us find a handful of surgeons that would aptly be described as “likeable badasses;” they’re very good at what they do, but they are also easy to work with professionally and get along with their patients. So the question, it sounds like, is how do we get talented women—or anyone who is struggling with this—to be seen as a likeable badass?
AF: If you have a choice, you’re always going to want to refer to someone who is both likeable and a badass. Anyone who is low status is probably going to be stereotyped as only one or the other. Either you’re really caring and have great bedside manner but I don’t think you’re that good at what you do, or you’re really great at what you do but I think you’re a total bitch.
So what I talk about a lot in the book is acting deliberately and quickly at the outset of a relationship while people aren’t thinking much about you. Whether it’s gender, race, ethnicity, or you speak with an accent, biases are stacked against you. Take people’s minds off that bias and turn it to the way you’re showing up, whether that’s how you’re talking about yourself or how others are saying great things about you.
Here’s an example. Imagine a woman you’ve never met, but someone you think highly of says about her “Hey, you know she is really someone you should be sending your patients to.” Now, all of a sudden when that woman who you’ve never met does show up in your world, she already has status that has been built by a third party. Before you’d even started to think about her, something else had happened to make you think about this person as a highly competent and very caring person.
The advice I give then is that if you can get other people to do that for you, what happens is that you don’t even have to think about how you’re perceived by others, and you can just put your head down and start doing the work. Otherwise, you’re stuck trying to dig yourself out of a reputation problem—even though it was one you don’t deserve—from existing biases.
It’s kind of like the concept of preventing disease being easier than curing disease. If everyone in my family has had a heart attack in their 40s, am I going to wait until I have my heart attack and then say now that I’ve had my heart attack, I’m going to do something about it? Or would I say that statistically, I’m the kind of person that could have a heart attack, so I’m going to exercise more in my 20s?
The same logic applies here. The world has told us that women are at risk of problems related to gender bias, but we haven’t really been coached to do anything about it. So we go about our normal life, and a bad thing happens—a metaphorical heart attack. And we say “this sucks, now I have to try to heal myself.” And you can heal yourself, but it’s a lot easier than never getting sick in the first place. So what I talk about in the book is how to start building your status long before you ever need it, so you don’t end up in the situation where you have to change someone’s mind. Changing someone’s mind is possible, but it takes a tremendous amount of work.
CW: So what you’re saying is that when someone is developing a first impression, they’re going to succumb to various sorts of confirmation bias based on what they’ve heard before, so you should want to do everything you can to make that bias confirm good, positive things.
AF: 100%. One little bit of information can change the way you perceive someone else in just a second. I don’t know if this has ever happened to you where you’ve interacted with someone and you had no idea who they were, but then they say something and you realize that this person is a “big deal.”
For example, I do a lot of work with the military, and there are retired generals out there who are now civilians, wearing civilian clothes, and there are enough of them that no active duty soldier would know who they all are. And they might introduce themselves to someone who is active duty who asks “What do you do?” and they’ll respond “Oh, I’m a retired Lieutenant General,” and all of a sudden you can see their whole demeanor change instantly.

Of course, not everybody has the luxury of just dropping their high status occupation, because they may not have one. But there are things that I cover in the book that you can do to be able to say “I’m a person of value.” Let’s take the simple example of making introductions. Introducing people to each other is a competent and caring move—you’re competent because you’re connected, and you’re caring because you’re using your network to help someone.
Even if you’re in a lowly position in a hierarchy—like a med student—you can show people you have value. “Here’s an article I read that I think everyone could benefit from, so I’m emailing it out.”
Or when I was in grad school, there was the tediousness of reformatting research citations in various formats. It wasn’t hard work, but someone had to do it. So one of the things I did when I was a graduate student was just memorize the various citation formatting rules—should you write your citation this way or that way. It was nothing that someone else couldn’t have done, but nobody was going to take the time. All of a sudden I was a grad student that people needed to talk to. “Go talk to Alison, she knows the answer.”
So you can show up as the expert in something and you can solve someone’s problem. You don’t need to be a retired 3-star general for someone else to say “that’s valuable” or “I’m interested” about what you have to say.
CW: Certainly as a medical resident, one of the best ways to build a good reputation is by knowing how to get X, Y, or Z done around the hospital. And then you build that reputation of “oh yeah, he knows how to get that patient an x-ray sooner” or whatever.
AF: Those are things that you don’t need to have a fancy title to do, and sometimes not having the title can make it a lot easier. People feel sorry for you, they want to do you a favor; they don’t feel like they have to say yes to you so they’re more willing. So the whole idea is figure out ways to use your skills for someone else’s benefit in a way that doesn’t cost you a lot of time, and you’ve figured out a way to gain status. Then you can start to think bout building your status more broadly.
CW: One last question. We talked earlier about doctors and patients. Patients often come in as “low status” and “low power” within the healthcare system, and some patients have even lower status because of existing biases. You don’t have to look too hard to find evidence of bias where doctors are not believing things their female patients are telling them, not taking complaints from patients of certain races as seriously, and so on. In this very fragmented and dysfunctional health care system we have, I think patients are probably wanting both status and power. They want to feel like somebody cares about them and their complaints, and they want to have agency over what happens to them. Off the top of your head, are their any pieces of advice you might have for a patient who has an issue but doesn’t feel like they’re getting what they need out of the health care system?
AF: One simple one that comes to mind is to use an agent. I’m sure you’ve had this situation where a very elderly patient comes in and having trouble communicating, and you’re wondering what’s going on with them. Then all of a sudden, their child comes in who is very on top of things and is able to say “here’s what’s been going on, here’s what’s different than usual, I’m going to give you all of their records” and so on.

That child is their agent, and the patient benefits from their agent’s status as someone who is a trusted source of information. So if you’re not getting the outcomes that you want, ask who might be better: my neighbor, my husband, my child, or somebody else who might be able to help you get your needs met.
Sometimes it’s also helpful to bring in an agent when the patient is someone who is generally not very easy to deal with. If you’re the physician, you want to be able to take the person’s complaint seriously, but at the same time, physicians are human beings. When people are a pain in the ass, it doesn’t really motivate you to want to lean into helping that patient. But when you have those patients you just love and adore, you’re going to want to put in the extra effort to get the test done faster or relief sooner because you like them. So agents can be really helpful in helping with both the competence and the benevolence pieces of the relationship.
CW: In my experience, that agent can really be anybody who is essentially functioning as a third party who is listening to the conversation, watching out for discrepancies where the patient and the doctor might be talking past one another.
AF: One of the things we know about research on negotiation is that women don’t get as good of outcomes when they’re advocating for a benefit for themselves compared to when they’re advocating for someone else; for men the difference isn’t as big.
When you’re a patient, you’re advocating for yourself. You might still feel sick in the hospital and say to the doctor who wants to send you home, “I don’t want to be discharged today.” But it’s a lot easier to make that same request for someone else. Because of the status dynamics, it can be hard to ask for things for yourself. Other people can do it in a much more forceful way, because it’s not their life. When they’re saying “no” to going home, they’re not being selfish because they’re doing it for someone else.
CW: At many hospitals, there is a patient advocacy team, where someone can accompany a patient who could benefit from an agent when they’re talking with doctors. It sounds like we should have a very low threshold to suggest them when it seems like the patient and the medical team have a dynamic that isn’t working. What are some other ways physicians can give status to our patients?
AF: Simple things. People want to know their words matter, that they’ve been heard—so anything that says “I hear you.”
I remember one time my daughter’s back was hurting after she went jumping on a trampoline, and it wasn’t getting better quickly, so I asked if she thought it was bad enough to have to go to the doctor. And she goes “I don’t want to go to the doctor and have them tell me nothing’s wrong with me and feel dumb.” Human beings feel that way all the time—they want to be seen as competent.
So one way to honor people’s status is to say things like “trusting yourself and coming in was a smart thing to do.” Ask yourself: What would make the patient feel respected in this situation? What is this person probably worried about, and what could I say to them so that they feel like they’re a good person—a smart person—who is doing the right thing?
CW: Well thank you so much for chatting with me. I really appreciate your taking the time to focus on these issues in the medical field!
AF: For sure!
“Likeable Badass: How Women Get the Success They Deserve” by Alison Fragale comes out on September 3rd and is available now for pre-order. Also, for more from Dr. Fragale, check out her newsletter, “The Upper Hand.”
The average person needs more truth to make choices for themselves and their family. The truth in medicine seems to be elusive.